Bench Press Sling Shot by Body Reapers

Injuries around the elbow pose a challenging problem for orthopaedic surgeons. The complex bony architecture of the joint should be restored and the thin soft tissue envelope needs to be handled with meticulous care. Elbow instability is a complication seen after dislocations and fractures of the elbow and remains a treatment challenge. The purpose of this study was to provide subjective and objective results following the surgical treatment of unstable elbow dislocations with an external hinged fixation technique Elbow Wraps.

Forty-six consecutive patients with complex trauma of the elbow with instability after ligament reconstruction were enrolled between January 2017 and December 2019. The parameters used to quantify the subjective and objective functional results were the Mayo Elbow Score (MES, objective) and Oxford Elbow Score (OES, subjective), and clinical stability of the elbow joint. We also performed a radiological follow-up of the fractures.

The mean MES and OES scores were good at the 12-month follow-up. We had 38 patients with stable joints and 8 patients with minor instability. Using the stress test, we saw a significant difference in the affected joint under varus stress (6.7 ± 1.8 mm) compared to the healthy joint (5.8 ± 1.2 mm) laterally. Furthermore, medially the gap was significantly larger (5.8 ± 0.8 mm, treated elbow) than the contralateral gap under valgus stress (4.3 ± 0.8 mm) (p <0.001). Twenty-one complications occurred in 46 patients (46%): Seven patients had a clinical change of elbow axis: Three valgus (6%), four varus (9%); Superficial wound infection occurred in one case (2%) and ulnar nerve dysfunction in two (4%). The most common medium-term complication was post-traumatic osteoarthritis in eight cases (17%). Heterotopic ossification occurred in five patients (11%) and elbow stiffness in five cases (11%).
The use of the hinged elbow external fixator in the treatment of complex elbow trauma is a valid therapeutic adjunct to ligamentous reconstruction showing encouraging results with acceptable complications.
How to cite this article
Meccariello L, Caiaffa V, Mader K, et al. Treatment of Unstable Elbow Injuries with a Hinged Elbow Fixator: Subjective and Objective Results. Strategies Trauma Limb Reconstr 2022;17(2):68–73.
Injuries around the elbow pose a challenging problem for the orthopaedic surgeon.1 The complex bony architecture of the joint should be restored and the thin soft tissue envelope requires meticulous care.1,2 Fracture fixation and ligament repair should be stable enough to permit early postoperative mobilization to prevent post-traumatic stiffness and pain.3,4 In fracture-dislocations with severe soft tissue swelling, the risk and benefit of an extensive approach need to be weighed against a less invasive method providing adequate stability to allow early postoperative joint mobilization4 (Figs 1 and 2).
Figs 1A to M.
(A to C) Clinical photographs of a 48-year-older man with an open elbow injury, radial nerve palsy and metacarpal injuries on the left side; (D and E) The 3D-angio CT showed the elbow dislocation without arterial injuries; (F and G) The hinged external fixator is in place with an extension to the wrist; (H to J) The postoperative CT showed the reduction of radio-humeral and ulnar-humeral joints; (K) After 2 weeks we unlocked the hinged external fixation from the wrist external fixation; (L and M) Radiographs showing good reduction after 6 weeks of use
Figs 2A to E.
(A and B) Twelve months after surgery on the left side, the radiographs showed fracture healing of the elbow and wrist and little bone metaplasia around the MCL and LCL; (C to E) The elbow had a good range of motion, yet the radial nerve palsy persisted
This is not always possible in cases with open fractures, a floating elbow (Fig. 1), multi-ligament injuries with soft tissue damage, polytrauma, irreducible elbow dislocations, or in the elderly population where internal fixation is further compromised by demineralized bone.1–6 One of the most common problems encountered is elbow instability, which may arise through chronic overuse syndromes or as post-traumatic sequelae.4–6 Patients with chronic instability classically present with pain, apprehension, or mechanical subluxation of the elbow joint. External fixation appears to be an appealing adjunct to minimal surgical intervention, as it protects the fixation required and provides adequate stability to the joint for early postoperative motion around the rotation arc7 (Fig. 3).
Figs 3A to M.
(A) Seventy-year-old female had a left elbow posterolateral dislocation with an intra-articular fracture of the capitellum after a low energy trauma; (B and C) After reduction and casting in the emergency department, the CT showed the fracture and persistent elbow dislocation; (D to F) In the acute setting, we performed surgery with osteosynthesis, and applied a hinged external fixator; (G) Postoperative clinical image; (H and I) After 12 months radiographs showed good elbow alignment without osteoarthritis; (J to M) Excellent clinical outcomes after 12 months
The aim of the study was to evaluate a group of patients in whom external fixation was used as an adjunct to manage severe injuries to the elbow, including unstable dislocations, fracture-dislocations and chronic instability and to provide subjective and objective results utilizing this technique.
From January 2017 to December 2019, all consecutive patients with acute instability, dislocations and fractures of the elbow joint were registered from three Italian Trauma Level I Centres and screened for this study.
From these fractures, we excluded patients with other injuries according to the characteristics described in Table 1.
Inclusion and exclusion criteria
All injury types were classified using plain radiographs and CT scans.5–7 The patients were informed in a clear and comprehensive way about the type of treatment and other possible surgical and conservative alternatives. Patients were treated according to the ethical standards of the Helsinki Declaration and were invited to read, understand, and sign the informed consent form.
In all cases, we applied a hinged elbow fixator using the Cittieffe hinged elbow fixator (Calderara di Reno, Bologna, Italy). All patients underwent the same rehabilitation protocol, starting active flexion and extension on day 5, with periodic follow-up examinations, frame stability checks and regular pin site care. After 6 weeks, the external fixator was removed, and full passive and active movement of the elbow was allowed. From 12 weeks, the patients commenced light upper extremity weight training and started an endurance programme simulating desired work requirements.
The patients received indomethacin 75 mg once a day for 4 weeks to prevent heterotopic ossification.8 To study bone healing on radiographs, we used the Non-union Scoring System (NUSS) in retrospective mode.9
The criteria to evaluate the injured elbow with a healthy elbow during the follow-up were the duration of surgery, objective quality of life and the elbow function measured by the MES,10 the subjective quality of life and the elbow function measured by OES10 and the clinical stability of the elbow joint. In addition, we measured the medial and lateral joint space by varus and valgus stress ultrasound examinations of the elbow.11 The elbow alignment was measured using the trochleocapitellar index in adults as described by Rollo et al.10 This is a ratio between the angle of the capitellum and the trochlea. Bone union was measured using the radiographic union score as described by Whelan et al.12 The evaluation endpoint was set at 12 months after surgery. Longer follow-up was performed when possible, to detect complications occurring after the evaluation endpoint, such as early post-traumatic osteoarthritis.
Descriptive statistics were used to summarise the characteristics of the study group, including the means and standard deviations of all continuous variables. We compared the injured side to the uninjured, healthy side as an in-patient control. The t test was used to compare continuous outcomes. The Chi-square test (subgroups of 10 patients or more) or Fisher's exact test (subgroups smaller than 10 patients) were used to compare categorical variables. The statistical significance was defined as p <0.05. We used Pearson's correlation coefficient (r) to compare the correlation between the patient-reported outcomes and quality of life.
The reliability and validity of the correlation between functional outcome results and the trochleocapitellar index were determined using Cohen's kappa (κ).
Forty-six patients were treated, of which 32 were male and 12 were female. The mean age was 43 years (range 16–93 years). The left side was affected in 25 cases (54%) and the right side in 21 cases (46%). The average duration of follow-up was 28 months (range 12–36 months). A fall from a height was the most cause of injury. There were 38 closed injuries and five compound fractures. Further demographic details are described in Table 2.
The lateral collateral ligament complex (LCL) was injured in 23 cases (50%) (Table 3), the coronoid acting as the primary bony static stabilizer was involved in 17 cases (37%), and there were 14 (30%) cases with avulsion of the common extensor origin tendon. There were two (4%) ulnar nerve lesions. The average Injury Severity Score (ISS) was 3.5 (range 1–24) and the average Glasgow Coma Score (GCS) was 14 (range 7–15).
The mean surgical time was 87 minutes (range 21–123 minutes). The time to complete bone union was 87 days (range 59–112). In patients with intra-articular fractures, we observed 28 different complications, the most common being post-traumatic osteoarthritis in eight cases (17%). An overview of outcomes is listed in Table 4. At 12 months after the surgery, the average arcs of flexion-extension and pronation-supination were statistically worse on the injured sides (p <0.05). Varus and valgus stress showed an increased widening of the joint spaces on the injured sides (p <0.05).
Comparison of outcomes for the injured and uninjured elbows
Collateral ligament tears were sutured with either an anchor (25) or with a transosseous suture, and nine cases required osteosynthesis utilizing plate, cannulated screws or K wire fixation. The quality of life and elbow function immediately after treatment of the injury with external fixation, measured using the MES, was 64 points (±25; range 26–100) for the injured sides, and 95 points (±3; range 90–100) for the uninjured side. After 12 months, the MES increased to 75 points (±16; range 42–100) while the uninjured side remained stable at 95 points (±3; range 90–100).
The subjective quality of life and elbow function with the external fixator, measured using the OES, increased from 66 points directly after treatment (±26; range 22–100) to 71 points (±25; range 36–100), as the uninjured side remained stable at 92 points after treatment (±6; range 84–100) and 92 points after 12 months (±8; range 78–100).
In total, 21 complications occurred in 46 patients (46%): Seven patients had a clinical change of elbow axis [three valgus (6%), four varus (9%); superficial wound infection occurred in one case (2%) and ulnar nerve dysfunction in two (4%)]. The most common medium-term complication was post-traumatic osteoarthritis in eight cases (17%). It is unknown whether this is a direct result of the initial trauma, and how external fixation stability affects the natural history of post-traumatic osteoarthrosis. Heterotopic ossification occurred in five patients (11%) and elbow stiffness in five cases (11%) (Table 4). The residual joint instability with approximately 1 mm of extra joint widening of the affected joint is statistically relevant yet clinically less relevant as this did not result in gross instability of the elbows.
A fracture-dislocation of the elbow joint is a complex injury, which requires anatomical stable reduction to maintain well-aligned articular surfaces and prevent joint instability and additional soft tissue insult. These injuries are notorious for sequelae such as instability, rigidity and early osteoarthrosis.
Indications for the use of an articulated external fixator include acute instability, instability after osteosynthesis or ligamentous repair, chronic subluxation, open fractures, fracture-dislocations in uncooperative patients and complex injuries in the elderly population. We have used external fixation in patients with elbow instability, fractures and dislocations with good results,13 and several publications have reported on the use of hinged external fixation in the treatment of both acute and chronic elbow instability.13 Yu et al. reported the outcomes of 20 cases with acute complex instability of the elbow treated with hinged external fixation.14 Interestingly, these authors did not repair the LCL when using a hinged external fixator.13,14
In our series, the most common soft tissue injury was the LCL complex, and the coronoid was involved as the most frequent bony injury of the elbow together with radial head fractures.13
Our series and the literature support the use of articulated external fixation combined with minimally invasive fracture repair or ligament reconstruction, avoiding the need for an extensive approach required for a formal repair of the affected ligaments, as the hinged fixator protects minimal repair from excessive strain. This facilitated early recovery and effective early rehabilitation and movement. This aims to prevent scarring and stiffness in these patients.14,15 It is not possible to review post-traumatic elbow instability due to fracture-dislocation while ignoring the osseous injury, and the results of different fracture patterns are difficult to compare. We focused on the treatment of the ligamentous structures of the elbow joint and excluded patients with larger osseous lesions. To the best of our knowledge, this is the largest study about the use of a hinged elbow fixator for isolated ligamentous injuries of the elbow joint.
Attention to detail remains vital when applying the fixator, as complications can occur if anatomical safe zones are not respected. Osteoporotic bone or compromised soft tissues are often seen in the elderly population, which can affect the outcome of surgical reconstruction. In such circumstances, the hinged external fixator becomes an invaluable adjunct offering added stability to permit early joint movement. It is also now possible to limit the surgical approach to obtain optimal joint reduction with minimal internal fixation. Simple realignment of the metaphyseal fragments utilizing the fixator, if properly applied, can neutralise all the dislocating forces around the elbow.16 Hinged elbow fixators have been used in cases where residual instability is seen after ligament repair or fracture reduction.11,17
The medium-term range of motion and subjective results, as shown in this study, support the validity of hinged elbow fixation in acute elbow injuries combined with the ligamentous repair. This device is tolerated well by patients when applied correctly, and the potential complications with external fixation are manageable. External hinged fixation is a stable and effective method, which could significantly improve the treatment outcomes and reduce wound complications for ligamentous injuries around the elbow. It does however rely on careful patient selection, attention to detail in its application and a specific follow-up protocol to achieve good short- and long-term outcomes.
Source of support: Nil
Conflict of interest: None
Categorias
Leia mais
Comprehensive Outlook on Executive Summary Colorants Market Size and Share CAGR Value Data Bridge Market Research analyses that the global colorants market, which was USD 37.04 billion in 2022, would rocket up to USD 52.12 billion by 2030 and is expected to undergo a CAGR of 4.36% during the forecast period of 2023 to 2030. This competitive era calls for businesses to be equipped with...
"Executive Summary Surgical Operating Microscopes Market Size and Share Forecast The global surgical operating microscopes market size was valued at USD 1.84 billion in 2024 and is expected to reach USD 5.80 billion by 2032, at a CAGR of 15.40% during the forecast period Surgical Operating Microscopes Market business report is a...
"Executive Summary: Enterprise Resource Planning Technologies Market Size and Share by Application & Industry Data Bridge Market Research analyses that the global enterprise resource planning technologies market which was USD 3,231.41 million in 2022, is expected to reach USD 67,172.04 million by 2030, and is expected to undergo a CAGR of 46.1% during the forecast period...

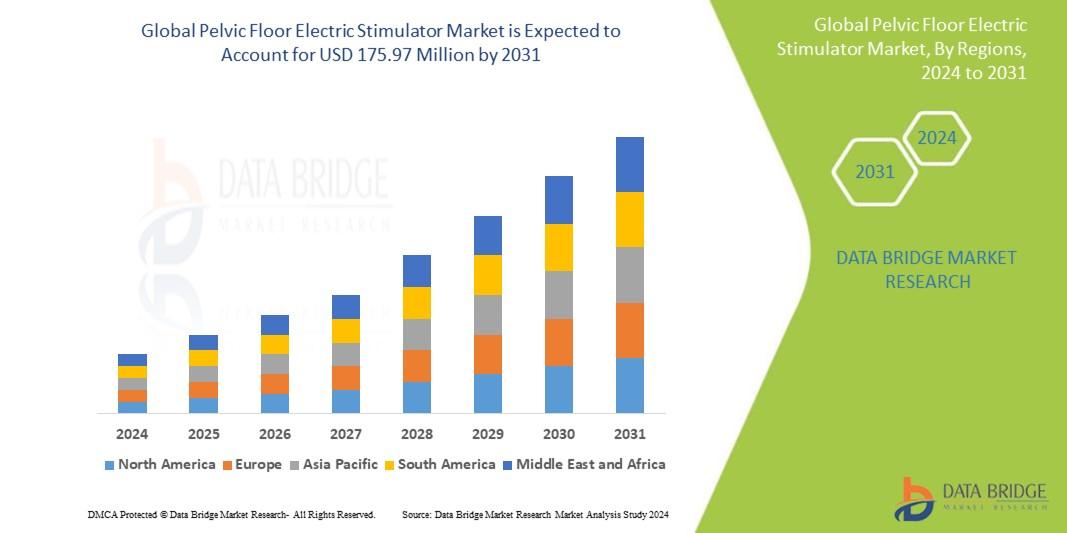
"Detailed Analysis of Executive Summary Pelvic Floor Electric Stimulator Market Size and Share The global pelvic floor electric stimulator market size was valued at USD 102.87 million in 2024 and is projected to reach USD 187.05 million by 2032, with a CAGR of 7.76% during the forecast period of 2025 to 2032 In the universal Pelvic Floor Electric Stimulator Market research report,...
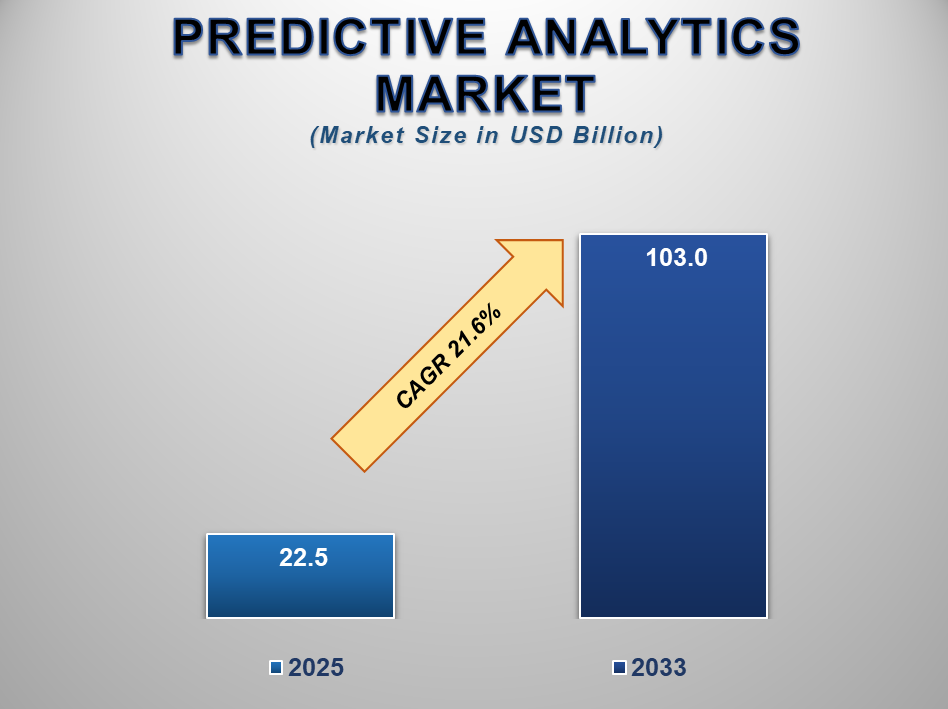
Predictive Analytics Market Overview The Predictive Analytics market is anticipated to grow significantly from 2025 to 2033, fueled by the increasing need for data-driven decision-making across industries. By 2025, the market is projected to reach a value of around USD 22.5 Billion. Looking ahead to 2033, it is expected to expand further to about USD 103.0 Billion. This...